
Week 2 in Rwanda
Day 8: Sunday March 12, 2023
After sleeping in another morning this weekend, we went back to our favorite local coffee spot - Question Coffee. They just have such nice views and really good coffee, making it a no brainer especially when it’s a quick 3 minute walk from our place. After a light breakfast with banana bread and lemon cake, we headed up to a hotel to see if we could get a taxi to Mount Kigali. This was one of the local sites that people had been telling us to see. And it lived up to the hype. We were determined to do a little hiking today. Our taxi driver took us to the Welcome Center for the mountain where they had lots of activities for kids and an opportunity for get a guided tour. We were feeling adventurous enough to figure out the route on our own and we quickly found exactly where we needed to go. The beginning of the hike was pretty dusty and hot, but after about 10-15 minutes of walking we entered this forest area that was like a sanctuary. Between the shade and the breeze, it felt like mother nature’s version of air condition. The air in this area seemed to be more pure and filled with oxygen. As we walked through forest, we first ran into a group of people that looked like they were filming some type of project. One person had a camera, another had a long microphone, one person was carrying a guitar, and the person in the center of it all was painting a portrait of trees using sunset colors (different shades of red, orange, and yellow). They were extremely friendly people and told us that they were filming a movie. As we continued down further into the forest, we eventually reached the look out point that Danny remembered from last year. This had some breath taking views of the massive rolling hills throughout the center of Kigali. You could truly appreciate all the peaks and the valleys and all of the communities that built houses along the steep terrain. We continued to hike around Mount Kigali and ran into more people along the way - one group of tourist was being led by “Mr. Kigali” who was Shyamal and Danny’s city tour guide from last year. We also ran into a lady who was working in the heat with the sun beating down on her as she was breaking up rocks and stone for future construction projects. As we passed, she smiled and waved at us as if nothing was bothering her. After hiking around for about 30 minutes, we made our way back to the sanctuary forest. Sara wanted to spend some time meditating here, so I introduced the group to the concept of “box-breathing”. This pattern of breathing is 5 seconds of inhaling, 5 seconds of holding your inhale, 5 seconds of exhaling, and 5 seconds of holding your exhale. The idea is that you can focus on your breathing if you feel your mind wandering but eventually you can get to a point where you are breathing without thinking and can absorb the sounds around you. After 5 minutes we all opened our eyes with a peaceful soul and a deeper appreciation for the forest around us.




Once we left Mount Kigali, we headed to the Convention Center. This was a building that you could see from pretty much any part of the city if you had the right elevation. At night time, you would see lights circling around the building with different colors, giving the illusion that the building itself was spinning. When we got there, we unfortunately couldn’t tour the facility because the FIFA conference was taking place that afternoon. They did point us in the direction of the Raddison Blue Hotel where we caught some respite and had some water, juice and snacks in their fancy hotel lobby. I asked the receptionist how much a night to stay here costs and she told me the cheapest room was $250/night and the most expensive suite was $15,000/night, which the King of Qatar had just stayed at recently and paid $20,000/night. She offered to have one of us tour the most expensive room but I wasn’t super comfortable seeing luxury like that in this setting so I politely declined.

After leaving the hotel, we headed to the Genocide Memorial. This was one of the heaviest parts of the trip emotionally so far. The tour started with a 9 minute video interviewing survivors of the genocide who talked about the moments they escaped and how their families were left behind and attacked by the Hutus. I was filled with sadness hearing and reading about how neighbors and friends (including children) would turn on their neighbors and give up their hiding spots with the goal of eliminating Tutsis from Rwanda. And then my sadness turned to anger realizing that genocides like this don’t just spring up overnight and much of the hateful speech and thinking came from years of Belgium propaganda creating hate between these two groups. The next overwhelming feeling was realizing that the international community, include the US, completely ignored what was happening in Rwanda and delayed their aid to help end the genocide. It is truly remarkable when you think about how recently this all was and how welcoming and appreciative the people of Rwanda are to foreigners. It’s heartbreaking to think that governments around the world allowed the killing and destruction of a country that they previously had interests in when it was convenient for them. It really made me reflect on what my role was in Rwanda this trip. My hope is that the work we were doing was empowering for Anesthesia trainees to continue to improve the healthcare safety and availability in their home country.
After debriefing a bit amongst ourselves on the ride home, we started to make dinner plans. We first stopped by a local art cafe that wasn’t too far from our ultimate dinner destination. We ordered juice and African tea at the cafe and walked around the art gallery as we waited for our drinks. The artwork had themes of women empowerment and generational connections amongst Rwandans. The pride for their country certain stood out in the artwork. We met someone who was a photographer and protege of the main artist for the cafe. He showed us some of his photographs of various musical artists that played at their local Kigali venue. Once we finished our juices, we headed to a traditional East African restaurant called “Chez John”. The menu was a bit difficult for us to decipher so we ended up asking our waiter to bring out enough dishes that would allow us to eat family style with different styles of meats and sides. He did an excellent job bringing out delicious food with the perfect portion sizes for our group. We all left with bellies full of new flavors and dishes we had never tried before.


When we returned home for the night, Sara and I taught Danny Monopoly deal. There was a similar progression for Danny that I saw Shyamal and Sara go through where it took a few rounds to get a hang of the rules. But once they tasted victory their competitive side came out. With Danny, Sara and I didn’t hold back in the first few rounds. We were stealing all his cards and making him earn everything in the game. This definitely helped to bring out his competitive side and once he finally won it was the most excitement I had seen from him in a long time. We played a bunch more rounds until we all got tired. Ending the night with card games is one of my favorite ways to connect with a group of friends.
Day 9: Monday March 13, 2023
Today was our last academic day with all of the residents and the start of our last week in Rwanda, so we had to seize the day. We started by carrying the supplies we brought with us up 2 miles of hills to the hospital and gave them to the Anesthesia staff who help stock their work room. They were so excited to receive epidural needles, regional block needles, and double lumen tubes. After handing off the supplies, we attended morning report where the overnight resident presented a patient who sounded very septic, was in DKA, and ultimately remained intubated and on pressors in the PACU. This was the first morning report where most of the discussion was in French. It sounded like there were some very sensitive conversations happening with a few English words breaking through the French. Most notably phrases like “you should call me any time you feel uncomfortable” and “this could be malpractice” were being used. The resident I was sitting next to tapped me on the leg and said he’ll catch me up on the conversation after morning report was done. Ultimately, it sounded like a case of a patient who was inadequately resuscitated and had little to no pre-operative workup (most recent labs were from a few days ago) but had ended up in the operating theater for what was being considered emergent surgery by the surgical team. The biggest take aways from morning report was communication is key and preoperative assessments should never be taken for granted, even if the surgical team is rushing you to the theater.



The morning portion of the academic day revolved around MSK diseases and orthopedic surgeries. The residents continued their practice of dividing into 2 groups and collecting thoughts on the learning objectives for the day, then coming back to the full group to discuss and write out what we chatted about in our groups. I really like this form of lecturing because it gets the residents out of their chairs, keeps everyone engaged, and shifts the ownership of the material onto the learners. The best part is there seems to be no hesitancy or shyness amongst the residents when working together. After going over the three learning objectives, we then took a quick break before jumping into the case presentation for the second half of the morning session. Before the break, I made a quick announcement about the video project I had in mind that involved interviewing any resident that wanted to participate, asking them about 3 questions revolving around Rwanda and Anesthesiology. During the break time, Isaac quickly approached me and was the first eager participant for my project. After I interview him, it was time to gather again and finish up our case-based discussion before lunch.
When it was time for lunch, Justin asked to speak with me outside. I could tell it was about my project before he said anything. He wanted me to run the project by their program director, Dr. Francois, before going ahead and recording the rest of the residents. It seemed like a totally reasonable request, but since I hadn’t interacted much with Dr. Francois or know where to find her, I had Justin set up a quick meeting. We met her at the pediatric OR. Dr. Francois had a strong presence about her, probably based on the position that she held and the amount of work she was doing on a daily basis. Justin nervously explained to her why he brought me to her but I quickly took over the explanation knowing that this was my place to talk about the project I had in mind. After telling me that she wanted to see the final product before I did anything with it, she agreed to let me proceed with interviewing the residents. “I trust my residents will have the appropriate answers to your questions” she said with confidence. Justin had a huge sense of relief about himself. He told me now if anything went wrong he could not be blamed for anything as the chief resident. I was getting a sense that freedom of speech felt restricted in Rwanda, probably reflecting the authoritarian leadership in their government. My first question that I wanted to ask the residents - ‘why do you love Rwanda?’ - was something that Justin was concerned would come off as too political. But others, including Dr. Francois, seemed to think it would be ok to discuss. I simply wanted to bring some light to locals’ perspectives about their own country for an audience of people who probably only view Rwanda through the lens of “Hotel Rwanda”. This movie was certainly a huge influence on my perspective before coming here.
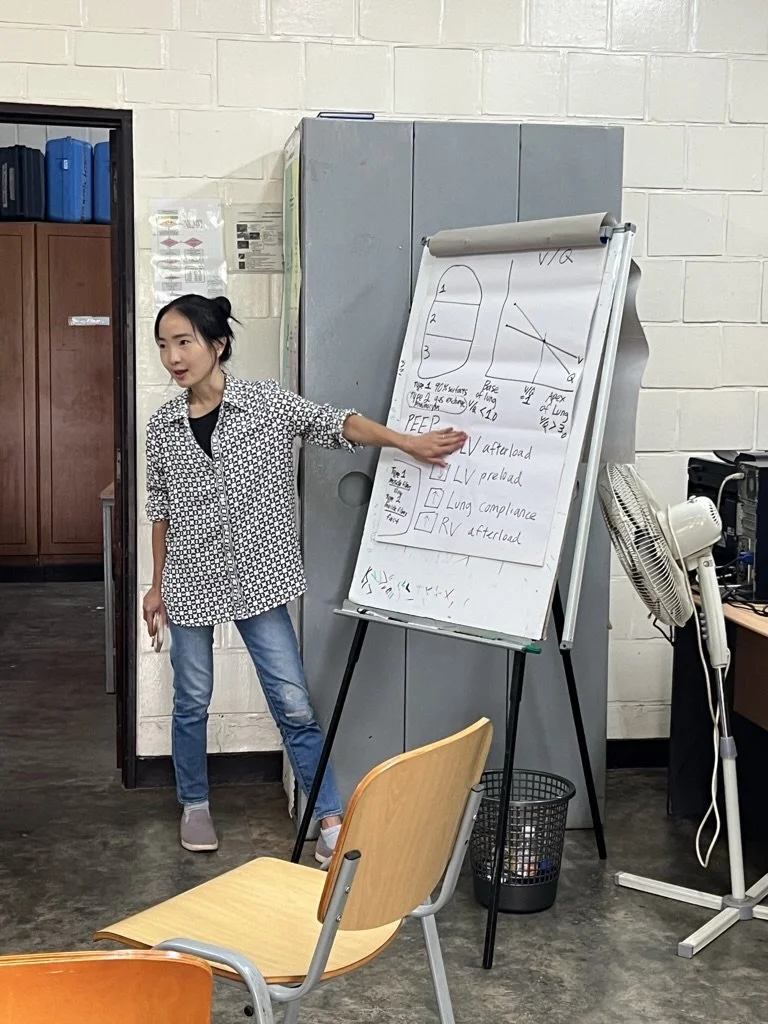
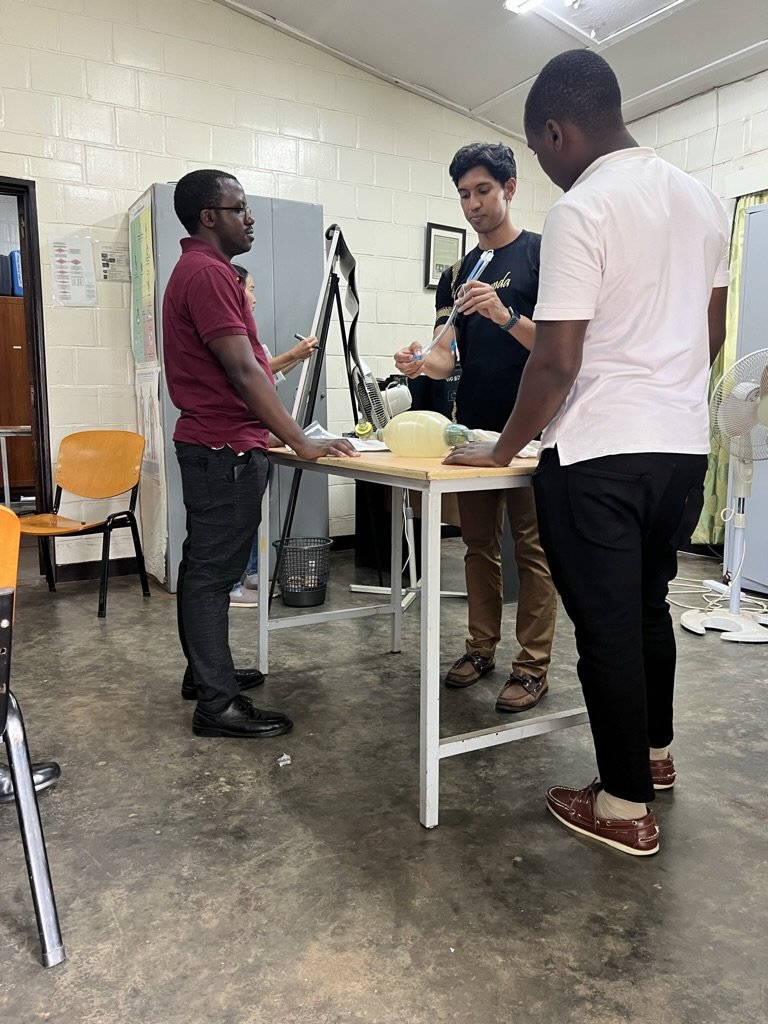
After our lunch break, we gathered back together for the afternoon portion of the academic day. Our goal was to discuss double lumen tubes and single lung ventilation. Sara started the lecture with chalk-talks about respiratory physiology leading into the indications and contraindications of single-lung isolation. After she was done I had the residents gather around a table while I went over the anatomy of a double lumen tube. Our original goal was to use one of the airway mannequins to demonstrate how to isolate the left and right lungs. Unfortunately the DLTs were unable to be passed through the vocal cords of the mannequin so we had to quickly pivot to another plan. So instead of doing a simulation, we decided to use Sara’s “Rapid Review for Oral Boards” book to go through a scenario of single lung ventilation. This was the first time they had been exposed to an oral boards style lecture and it seemed like they absolutely loved it. We ended up calling up a new resident for each question and every time we came to a new question, the next resident was eager to get into the hot seat. Sara and I did our best being an apathetic monotone oral board examiner and gave little feedback as the residents answered the questions. Once we got to the end of the scenario, we reviewed some of the questions that the residents had missed. Then we had Danny Bui conclude the afternoon session by going over his strategies for addressing hypoxia during one lung ventilation.


On our way home from work, we stopped at a Pakistani restaurant called Lahori for dinner. Danny and Asher had been raving about this place so I was excited to check it out. It was at the top floor of a corner building in a busy intersection. The restaurant was covered by a roof but the sides of the location were exposed to the elements. This became quite obvious once a rain storm started to come into town. It started as a subtle drizzle that didn’t seem to affect us much. But it eventually turned into a down pour with strong winds that blew the rain sideways, which started to get our tables, plates, and silverware wet. We moved to another table that was slightly further from the exposed edges of the restaurant. This seemed to solve our problem until we noticed that the floor was beginning to flood and our bags were getting wet. Another issue was the power had gone out so as the dark clouds came in and the sun set, we never were really able to see what our food looked like. But every dish was so delicious. Maybe our taste senses where heightened in a scenario where we were blinded to what it looked like and also being on the top floor of building during what felt like a natural disaster. When we asked for the bill and a box for the leftovers, I shined the light from my phone onto the leftover food and that was the first time we saw what we were eating. It was one of the most memorable meals of the trip so far.

When it was time to head home, we waited on the ground floor of the building as the rain continued to pour. We were hoping to find a taxi that could take us the short distance home. While we were waiting, Sara asked someone if they could help us grab a taxi and this man almost immediately ran into the pouring rain to find a taxi for us. It was a remarkable act of selflessness. It didn’t take long to find a cab but we watched as he scurried from corner to corner checking cars to see if they were available, jumping around to avoid deep puddles in the street. I sat up front for the ride home and it was one of the most terrifying rides of my life. The car’s A/C was not working well enough to defog the front window so the driver would periodically wipe the windshield with a rag to improve visibility. Although there was only one really close call of getting into an accident, I was tensed up the entire ride as we maneuvered through the tight streets of Kigali with little to no visibility at times. Once we got home, we spent the rest of the evening playing more cards. I taught Danny another game called “Egyptian Rat Slap” but we ultimately came back to Monopoly deal and played that until we all tired out for the evening.


Day 10: Tuesday March 14, 2023

Today was our first day heading to the county hospital called King Faisal Hospital. It was known to be a bit more advanced and specialized compared to CHUK. We had to take a taxi instead of walking because it was a bit further from our apartment, closer to the Kigali airport. Once we arrived, the infrastructure of the hospital was notably impressive and modernized. We ran into one of the residents, Eric, who was able to show us where to change for the day. After changing into scrubs, we attending morning report where they discussed the overnight cases, which mainly sounded like a busy night in the OB department. One of the notable things in both the morning report at CHUK and KFH is that they both included prayer at some point during their meeting, giving insight into how much religion is incorporated into their culture.
After morning report, I went to the ICU to round with the KFH team for the day. One of the anesthesia residents, Justin, was able to show me around. There were two emergency medicine residents on the service as well. The first patient we were attending to was a male who was involved in a physical altercation resulting in a subdural hematoma. The patient was getting ready to be extubated. Justin and I discussed the extubation criteria from a head-to-toe assessment. The next two patients were pediatric patients in the same unit as the adults. The first patient was a girl who had Pott disease. When Justin asked me if I knew what this was, I embarrassingly had to say no and he explained she was suffering from one of the most extreme sequelae of extra pulmonary tuberculosis. The infection had reached her spine and started to create osteolytic lesions and scoliosis. She had already undergone her corrective spine surgery but was still recovering from a pulmonary and nutritional stand point. Her mother was at the bedside, feeding her spoonfuls of what looked like medicine mixed with flavored ice.
We also saw a patient that was a transfer from the neighboring country of DRC (Democratic Republic of Congo). He was the only Caucasian in the unit and there was little to nothing known about who this person was. There were only clinical signs pointing towards a mixed picture of cardiogenic and septic shock. In the past couple of days since he had arrived, he had been heading in the wrong direction and was getting sicker and sicker.
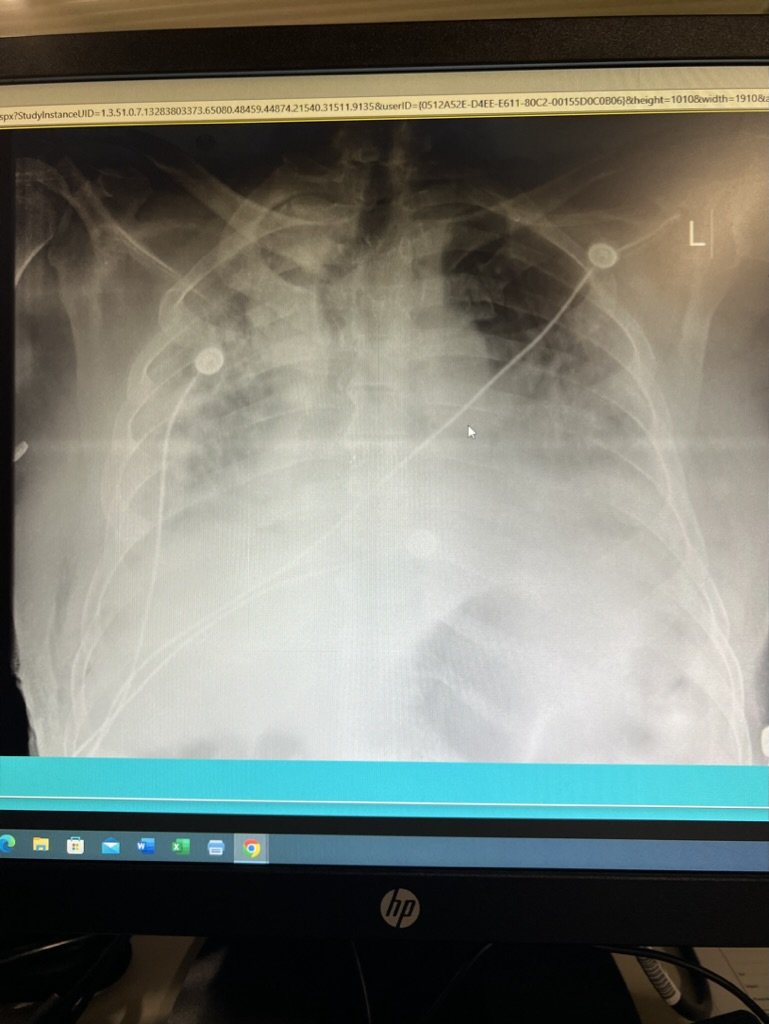
We wandered over to the other side of the unit, known as the HDU or “High Dependency Unit”. This was their equivalent of a step-down unit. We went to evaluate a patient who was suffering from hypoxia with his O2 sats hovering around the mid 70s until Justin came over and cranked up the oxygen to the max level possible. The ED resident grabbed the ultrasound and started to evaluate the lungs and heart. We gathered that this patient was suffering from pulmonary edema along with the IVC showing pretty severe collapsibility. The patient had recently undergone a lung biopsy but the diagnosis had not come back yet. A chest X-ray confirmed our suspicion of pulmonary edema and they placed the patient on BIPAP to help improve his oxygenation. He ultimately became too anxious wearing the mask and due to his intense work of breathing, the team elected to intubated him. While this was going on, there was a 4 month old patient who was post-op from a VP shunt and did not have any IV access. The patient was severely dehydrated and the team was struggling to find any locations for access. I suggested grabbing the ultrasound to see what veins were available but even with the ultrasound there was nothing visible that would be viable for an IV. When the pediatric team rolled around, they saw the team struggling to get access and suggested to switch over to PO hydration with an NG tube.

This was a bit of a defeating way to end the day, but afterwards I met up with Danny and Sara and we walked to a local spot for some lunch. It was a smallish cafe that was offering a lunch buffet for about $3. It seemed like it was full of people on their lunch breaks or who were finishing up work for the day in the nearby area. After we finished our plates, we walked towards the center of town and happened upon an ice cream shop. Given the heat at that time of the day, Danny and I both were interested in trying some of the ice cream and it hit the spot. After getting home for rest of the afternoon, there wasn’t too much for us to do so I was able to convenience Danny to go on a run before the rain came. The first half of the run, like always, consisted of running uphill for about 1.5 miles. Like the previous time, this portion was more of a jog-walk-jog-walk some more. Once we got to the flat portion of the town, we turned around and ran downhill back home. We cooled off outside the apartment and Danny and I had some conversations about how we see global health fitting into our future careers. I think it’s really powerful that Danny was able to and showed initiative to come back to Rwanda a second time. It proves that this experience can happen again if you put the time and effort into making it happen. Once the rain started to trickle in, we came inside and I put on a yoga video for us to finish our cool down with some stretching.

For dinner, we went to a Dim Sum restaurant that the group went to last year. It was a pretty westernized restaurant based on the prices and the international clientele that were there. We were meeting up with a medical student from UT Southwestern who Sara and Danny had run into at KFH. Her name was Sam and she was spending 2 months in Rwanda between her second and third year of medical school. She was working on a project that aimed to create an online app that would enable perioperative providers to enter medical information into a database that would be used to evaluate perioperative mortality in Rwanda . We met her at the restaurant and Sara and her immediately hit it off. They were talking almost nonstop about their passion for global health. Once we were done with dinner, we convenienced Sam to join us for some karaoke at our favorite local bar. Once she heard we would be going for our third time in a week, I think she was sold that she had to check it out. Everytime we have gone, the main singer does not disappoint. He was again dressed to the nines and was singing some classic love songs, giving the effect that we were are at wedding.

One of the funnier observations of the night was that we had gotten to Ikigai on the earlier side and he was all about having us sing the songs we requested. But as the night progressed, the placed filled in with more local Rwandans and again it seemed like everyone was more talented than the previous person singing. We knew it was our time to stop singing and just appreciate the beautiful voices around us. In particular, there was a group of 3 people who all came in at the same time. One singer first sang Ed Sheeran then sang a song in Kinyerwandan (the local language), both of which were beautiful but hearing him sing in his home tongue was magical. The second person was a girl who absolutely crushed a Whitney Houston song, showing off her incredible range. And finally the last person sang an English song that had a country twang to it and he absolute killed the vocals to it. There was no room for us to sing anymore after this display of talent, but it made for another fun and memorable night at Ikigai.
Day 11: Wednesday March 15, 2023
Morning report today was mostly a discussion about massive transfusions - how it is defined and what the potential complications are. Dr. Francois led the question-asking by starting with medical students, then residents, and ultimately asking me how we differentiate between TACO vs TRALI. It was a great refresher on the topic and is a good reminder that Anesthesiologists are experts in resuscitation, which becomes very relevant in obstetrics and trauma cases.
Our plan for the day was to join one of the residents, Robert, in the ICU for rounds. He told us rounds weren’t starting until 10am, so we took the time to have some African tea at a nearby restaurant. Now that I’m only a few months away from starting my critical care fellowship, I can truly appreciate how excited I am about starting that journey. I really enjoyed rounding with the team today and felt like I had something to offer educationally for almost every patient. The ICU was an 8 bed unit with all but one patient being ventilator-dependent. One of my favorite parts of the day was practicing POCUS on every patient. The best part was this wasn’t my idea - Robert wanted to scan everyone. I was able to give him some pointers along the way in terms of obtaining views and practicing a complete and systematic exam every time. For example, the biggest point of interest for him and the attending was looking at the IVC for volume status. But I continued to push him to do a full cardiac exam starting with the parasternal long-axis and ending with the subcostal view of the 4-chambers and rotating the probe 90 degrees to find the IVC. Our last patient had great echo windows and had some pathology that made for great discussion and direction for management. He was an elderly male who had been trached and was tachypnic while on supplemental oxygen via a t-piece. The team ended up putting him back on the vent to help reduce his work of breathing.



While Danny and I spent the day in the ICU, Sara had gone back to KFH to meet back up with Sam to learn more about her research project and see how she could help in the project. It sounds like it was a very beneficial day for Sara, making connections with the people of KFH and also the PI of the project who happens to a big name in Global Anesthesia in the US. By the evening time, she had received an email from this doctor that was very personalized and eager to work with Sara in the future after her fellowship training. This put Sara on cloud 9. Just another example on this trip of taking the steps of showing up to a situation and having things fall into place at the right time and right place.

When Danny and I left the hospital, we were hungry for a snack so we decided to stop at Lahori again. The owner recognized us from the previous night when it was catestrophically storming and told us to sit in the more sheltered part of the restaurant. After we ordered our food, the waitress also recognized us and invited us to sit inside what seemed like their only private room in the restaurant. I think they appreciated our dedication to come back. But honestly the food was so good, our natural disaster dinner could’ve been much worse weather-wise and we probably still would’ve come back. It was a good thing that we went into the private room because it started raining again while we were eating. After we were done eating, we scurried in the rain to the local grocery store to pick up some African tea and hot sauce to bring back home.
Once we got home, we passed some time before dinner playing cards and Farkle (a dice rolling game). The competitiveness of the group continued to heightened from the beginning of the trip. We were getting so loud that some of Sara’s shrieks made Danny’s watch give him an alert that he was in a loud place that was at risk for causing hearing loss. Once the rain had settled down a bit, we walked over to Ikigai, this time for dinner instead of karaoke. It was considerably more empty than we had ever seen it. I think at one point we may have been the only customers while we were eating. Their menu consisted of what we could consider bar food back home, but the quality and portion sizes (given the prices) were incredible. Danny and I both got steaks and fries that were delicious and we watch Sara put down a full chicken. We are really fortunate to have this location so close to our apartment especially since it’s been such a rainy week. The waiter has also gotten to accustomed to seeing us and gets so excited every time we come in. Knowing that this was probably our last time there, we grabbed a picture with him before we said see you later for now.



Day 12: Thursday March 16, 2023
Our last full day in Kigali was a packed one. We started the day by heading to the OB ward. We were invited to come there by Dr. Edward who was rounding in the ICU with us yesterday. When we arrived, we found him in one of the gyn operating theaters after they had just induced a patient who was having some tachycardia. After the patient stabilized from induction, he took us around the unit to show us the different areas such as the c-section room, L&D, and a make shift ICU room that was reserved for patients with severe peritonitis who would come from the district hospitals postpartum in very sick conditions. One of the things he was showing us in L&D was their epidural protocols that had been created by an Anesthesiologist from Duke. Dr. Edward said that a couple years ago he had created an epidural service but since he had been gone from CHUK for several months that service had died down due to lack of supplies. It seemed like something he was hoping to get started again in the near future. When we were in the c-section room, there was a UGH medial student there as well. We took the time to go over some topics related to spinal anesthesia such as properties of local anesthetics, dermatomal levels and block height goals for c-sections, and differential blockade.
After spending some time in the OB ward, I broke off the from the group to go to the ICU. There were only two residents rotating at CHUK this week based on everyone’s schedule and they were alternating 24-hour calls. So today William was there. The senior consult was the junior attending Angelic, who graduated from last year’s class. Rounds were disrupted this morning by a very very sick patient who came in hypotensive and was struggling to breathe. He had just been transferred to the HDU with the differential diagnosis of either severe tuberculosis and/or malignancy. Angelic did a remarkable job stabilizing and intubating him. After the intubation, a couple of the family members came back for an update. Most of this scenario was happening in French, but a lot of the actions that were taking place we not too far off from our own ICU practices and I’ve been in plenty of family meetings to know how that discussion was going.


After stabilizing this patient, we rounded on a few of the sicker patients and William practice his POCUS skills. It never got old watching their excitement to practice what they had just learned last week. The same patient from yesterday with pleural effusion and B-lines was improving slightly but still had recognizable pathology on ultrasound. After our break for lunch, William asked if I could walk him through placing an ultrasound-guided central line. He said he had done a bunch of blind ones since their other hospital sites didn’t have readily available ultrasounds like they do at CHUK, but had only done a handful with the ultrasound. When I came back from lunch, there was a family crying hysterically outside of the ICU. The patient that Angelic had resuscitated earlier in the day ended up passing away while I was gone. It wasn’t too surprising that this was going to be his ultimate prognosis based on how sick he was, but I think the timeline of it all took a lot people by shock. Even William seemed to be a bit distracted, scrolling silently through his phone while I sat next to him as they wheeled the body out from the ICU with the family close by. All it took was me asking him if he was doing ok and I think he realized how much his emotions were showing in that moment. He quickly jumped up and got back to work, gathering supplies for the central line. Even though I gowned and gloved up, he pretty much already knew what he was doing and needed very little assistance. The only real pointers I had for him was to stabilize his ultrasound hand with his pinky or ring finger to avoid collapsing the vessel with the pressure of the probe and to find the tip of this needle and position it in the center of the IJ once we thinks he’s in to ensure that it hasn’t gone through-and-through and to confirm that it’s not in the carotid artery before going in the with the wire. Then we used the ultrasound to confirm the wire placement before dilating the skin and neck muscles. From start to finish, the procedure must have been less than 10 minutes - impressive for a PGY2. But it sounds like at night time they are basically on their own and have to figure these things out on their own.

The rest of the evening was focused on networking for our last day in Rwanda. Our first stop of the night was meeting up with Angelic at a cafe called Camilla’s. There were multiple cafes with this name within a small radius in Kigali. Somehow Angelic and I found each other while we were looking for the correct one where Danny and Sara were. The two of them definitely found the best Camilla’s location which was located in a mall that we hadn’t been to yet. The restaurant was located on the top floor with a gorgeous view of the hills of Rwanda lit up by houses and street lights. Even at the end of the trip, I never got over how beautiful this sight was. Sara really wanted to connect with one of the few women attendings at CHUK so we got to know Angelic’s life pretty well after this meet up. I think it’s a valuable connection to make so that when Sara returns during her fellowship year, they can feel like they picked up right where they left off. Angelic clearly enjoyed showing off her kids and talking about life outside of work.
After meeting up with her, we headed to Khana Kazannah to meet up with a Partners in Health Global Health Fellow, Calum, who had been living in Rwanda for almost two years now. His main objective was working on the curriculum for the UGH medical students rotating through Anesthesia. Sam also joined us for dinner here. We had a live show at our dinner with what seemed like the wait staff and possible some additional singers, dancers, and drummers going through a variety of 15-20 minutes performances throughout our time there. The first time they paused, we thought that was it for the night and got into deep conversation with Calum about his life story. But once our food starting coming out, the performances started up again and the volume and stimulation was just too much to have dinner conversation. All eyes and ears were on these performers. At one point, they even had us stand up and join them in dancing. It was honestly a nice dinner break to make some room for more food. Calum had a pretty fascinating life and anesthesia training story, with plans of incorporating climate change mitigation and adaptation in the medical field for his future career goals.
Once we said goodbye to him for the night, Sam joined us back at our apartment for some card games. She picked up the game quickly and we managed to play quite a few rounds of Egyptian Rat Slap before there was an ultimate winner of the game. After listening to more about her story, she is definitely someone who has a bright future in global anesthesia, especially starting her current path at an early time in medical school. As we said goodbye to her for the final time, we encourage her to keep in touch along the way as she navigates the rest of medical school and gets closer to residency applications. I imagine our paths will probably cross again if all 4 of us continue to focus on global health in our careers. This focus within anesthesia certainly attracts a specific personality type and we all got along really well in such a short amount of time. With the Global Anesthesia circle being so small in the US, I image names and faces will start to come up over and over again as we seek out opportunities for research and outreach projects in the future.
Day 13: Friday March 17, 2023
Our final morning at CHUK. It’s always an odd feeling knowing that your time in a foreign place must come to a conclusion and you have to return back to the normal routine of life. All you can hope for is that the lessons and values you’ve gained on a trip like this can withstand the daily grind that is the healthcare system in America. Luckily I feel like I can rely on my colleagues who I traveled with to be supporting peers to check in with and reminisce on our time in Rwanda.

Morning report consisted of going over the overnight cases again. They had two cases of children swallowing coins and requiring an EGD - apparently also a very international experience. Then Robert presented on anesthetic management for aortic regurgitation which led to a discussion amongst the providers in the room. After the conversation wrapped up and everyone left, we said our goodbyes to Dr. Francois. She had a big smile ear to ear and thanked us repeatedly for our work the past two weeks. We emphasized that our time here showed that the program was in great hands and they were training amazing future Anesthesiologists for the country of Rwanda to provide safe and equitable surgical conditions for their people. She ended the conversation with “You guys are welcome anytime”, a simple but beautiful goodbye to 3 foreigners from the small state of Rhode Island.

We ended up coming home after morning report to nap and pack before starting our long journey home. It ended up working out perfectly because one we got home another severe thunderstorm rolled through town. After packing our bags, we had one more meal together. We walked up to a cafe called Indabo Cafe that was highly recommended by the previous CASIEF volunteer. This was our first time going but I’m glad we got to check it out. It felt like a cafe that was dropped in the middle of a rain forest. The rain certainly helped create the ambience, but the aesthetics wer on point there. We again had delicious meals even though I ordered something as simple as a chicken wrap. The three of us did our last bit of debriefing the trip and were continuing to talk about how we can carry the values and perspectives we gained on this trip back home. We also talked about how it can be difficult to convey just how your trip went without people having any reference point of what it’s like to walk around the streets of Rwanda and the hospital corridors of CHUK. We agreed to hold each other accountable to keep our attitudes positive as Sara and I finish our last 3 months at Rhode Island Hospital. We have bright futures ahead of us and it’s clear we can go even further when we do things together.