

Featured Posts



Looking for something specific?

Regional Anesthesia
As Anesthesiologists, post-operative pain control is a high priority for our peri-operative goals. Many patients are rightfully anxious about the pain they will be in after surgery. It is our job to create the best treatment plan curated for the specific patient and procedure involved. Over the past decade, we have incorporated a multi-modal approach to treating pain. This involves using a variety of medications that attack different receptors and act synergistically to reduce the overall dose needed to treat the pain and reduce the side effects that come with higher doses. Regional anesthesia refers to procedures that Anesthesiologists can perform that will help block pain to certain parts of the body. These techniques can help reduce the overall narcotics needed to treat a patient’s pain and allow a patient to get back to their daily activities sooner.

Oxytocin
Oxytocin is a hormone secreted by the posterior pituitary gland that has an effect on uterine contractions and breast milk excretion. It can also be created synthetically and is commonly used in obstetrics. It has dramatically decrease maternal morbidity and mortality from postpartum hemorrhage. For this reason, it is consider one of the drugs in the World Health Organization’s (WHO) list of essential drugs.

Difficult Airway Algorithm
One of our most vital jobs as Anesthesiologists is managing the airway. We are considered “airway experts” in the medical field. Without adequate ventilation and oxygenation after induction of anesthesia, your patients may deteriorate very quickly. Therefore, you must be prepared with an airway plans prior to putting the patient to sleep! The American Society of Anesthesiologists have developed guidelines to help physicians manage difficult airway scenarios. These scenarios can be stressful with very little time to fumble - knowing the key points of the guidelines will save you from being in a dire situation.

Hypoxemia
Hypoxemia and hypoxia are commonly used interchangeably as a way to describe a state of low oxygen levels. However, hypoxemia literally means low oxygen levels in a patient’s arterial blood (PaO2) and hypoxia refers to low oxygen levels in tissue. You can commonly see both if hypoxemia persists long enough, and you can also see them individually (ie. tourniquet applied to a distal extremity creating a lack of oxygen perfusion/flow). Monitoring oxygenation is one of our 4 major vital signs that we follow in the operating room. We can accomplish this three ways: a pulse oximeter, an FiO2 analyze, and monitoring the patients skin and mucous membranes for cyanosis.

Neuromuscular Blocking Agents
With the introduction of neuromuscular blocking agents (NMBAs) the overall goals of a general anesthetic expanded to include amnesia, analgesia, and now muscle relaxation. NMBAs are reserved for providers who are able to intubate and make airway interventions such as Anesthesiologist, Emergency Medicine, and Intensive Care Physicians. As Anesthesiologists, we primarily use NMBAs for creating optimal intubating conditions for laryngoscopy and airway management. We also use it for certain surgeries when it is extremely important that the patient does not move - for example, during robotic surgery when the arms of the robot are inserted into various laparoscopic port sites.
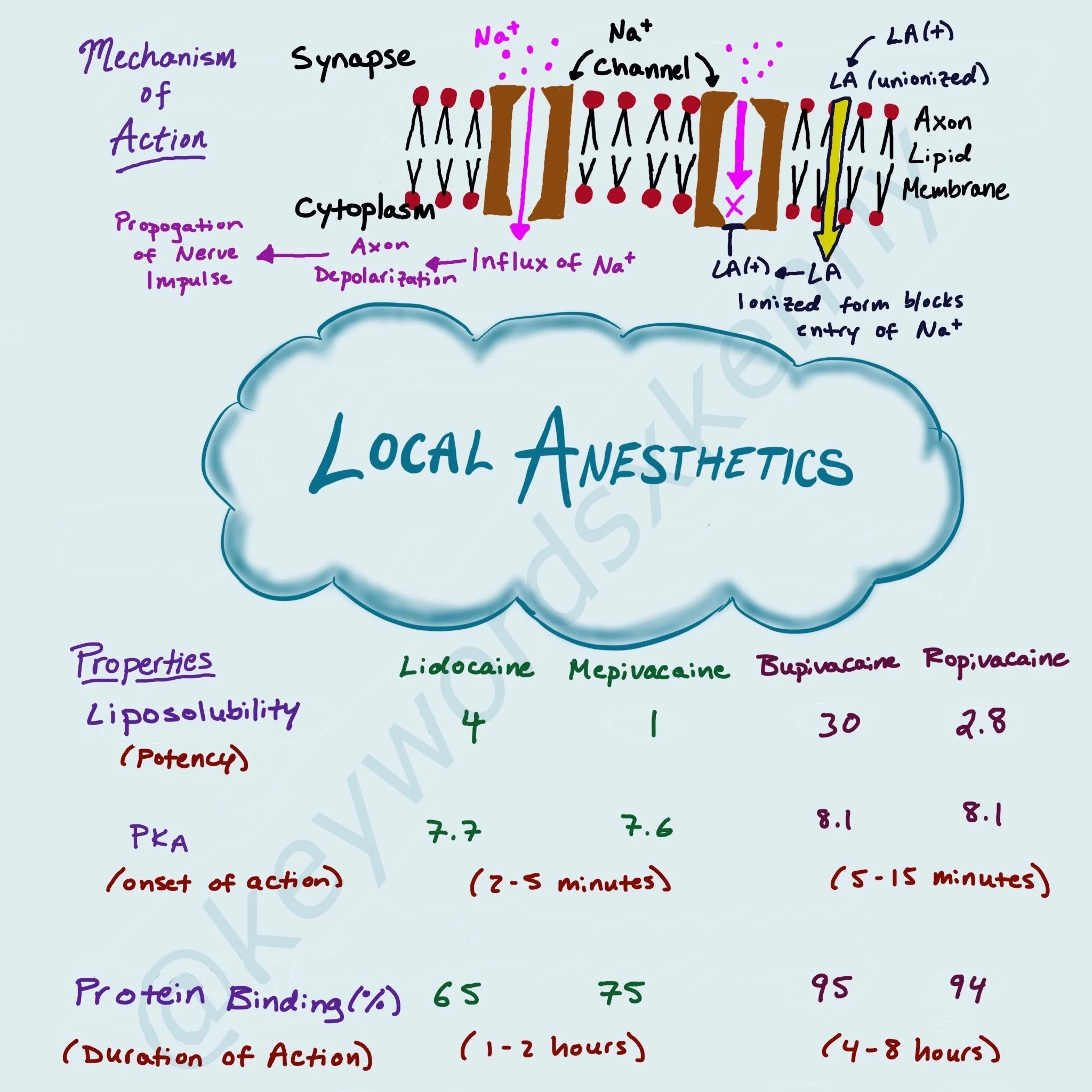
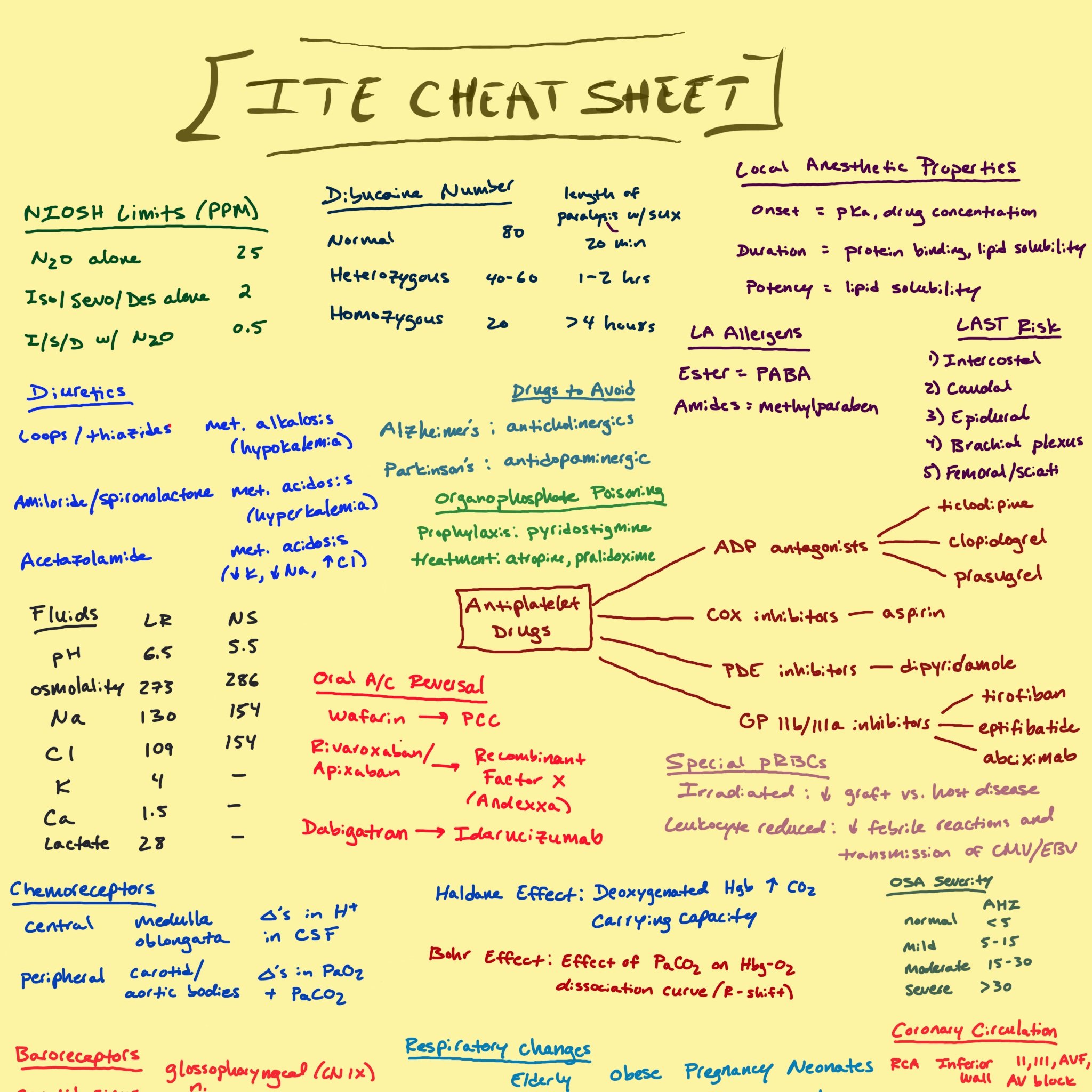
Local Anesthetics
Local anesthetics (LA) are used widely throughout medicine. Their purpose is to blunt the pain typically associated with some type of procedure. They are also one of the oldest known medications, dating back to the time of the Incas. We use a wide variety of different types and concentrations of LAs depending on their purpose. In Anesthesiology, we commonly use bupivacaine for regional blocks, epidurals, and spinals. We also use lidocaine subcutaneously when placing lines such as a central venous catheter.

Management of Hemodynamics
Referring back to the ASA Standard Guideline, anesthesia providers should be monitoring ventilation, oxygenation, temperature, and circulation. Hemodynamics is going to cover the circulation aspect for the patient. Majority of surgical cases with require some sort of hemodynamic treatment. Most often this is treating hypotension. But occasionally we also need to lower the blood pressure. Understanding how to compartmentalize the various components of hemodynamics will help you both diagnose the underlying cause of hypo- or hypertension and lead you to the correct treatment option.

Stages of Anesthesia
The defined “Stages of Anesthesia” is an old concept created by Dr. Arthur Guedel in 1937 that described the physiological changes patients would experience while being anesthetized with ether. Our ultimate landing spot is what we call “general anesthesia”, or a medically-induced coma with loss of protective reflexes. Prior to the development of modern day halogenated inhaled anesthetics and intravenous anesthetics, getting to the depth of general anesthesia was incredible dangerous from a cardiopulmonary perspective. These newer medications, along with new technology to monitor hemodynamics and ventilation, have made general anesthesia incredible safe. Let’s go through the 4 stages.

Opioids
Opioids have a long history in medicine dating back to the opium flower. Overtime, opioids have fallen in and out of favor for pain control, particularly post-operatively. In the past decade or two, we have unfortunately seen the rise of opioid-related deaths leading to an opioid epidemic of addiction and overdoses in the United States and worldwide. As dangerous as these medications can be, they maintain a crucial role in providing analgesia for surgical patients. In anesthesia, we administer opiates all the time for our patients, however, very calculated and cautiously. Based on the type of surgery, patient history, and post-operative plans, we layer narcotics into our multi-modal intraoperative post-operative analgesic plan. With a multimodal pain plan, you can limit how much narcotic a patient requires, reducing the side effects that come with these medications.

Minimal Alveolar Concentration
Minimal Alveolar Concentration (MAC) is a numerical scale that was created to correlate a depth of anesthesia with the amount of inhaled anesthetic that a patient is exposed to. The definition of MAC is the alveolar concentration of an inhalation anesthetic agent at 1 atmosphere (atm) and at stead-state concentration that is necessary to suppress a gross purposeful movement in 50% of patients in response to a surgical skin incision. Another way to look at MAC is it is similar to the effective dose (ED50) for medications. The potency of each anesthetic gas is inversely related to their MAC. The most potent gas, isoflurane, has the lowest MAC at 1.3%. Potency is related to the anesthetics lipid solubility (or oil:gas partition coefficient). The percentage of alveolar concentration is measured as the end-tidal concentration of gas. This is measured by the gas analyzer built into the expiratory limb of the ventilator. At a stead-state, the end-tidal concentration of the gas equals the alveolar concentration which also equals the central nervous system (CNS) concentration.

IV Induction Agents
Majority of patients (excluding the pediatric population) will come into the operating room with an intravenous catheter (IV). As anesthesiologists, we use this IV to get the patient off to sleep (induction) prior to securing their airway for a general anesthetic. We can also use an IV to administer boluses or continuous infusions of IV anesthetics to obtain various planes of sedation such as light, moderate, and deep sedation.

Inhaled Anesthetics
Let’s start with a history lesson. Nitrous oxide was first created in 1772 by Joseph Priestly - an English author, chemist, and minister. In 1799, nitrous oxide was used as analgesia for a dental procedure for the first time by Sir Humphrey David. It was used in America (Hartford, CT) for the first time by a dentist named Horace Wells in the year 1842. He used it on himself and discovered its hypnotic and analgesic effects. He arranged a demonstration at Mass General Hospital to show a painless dental surgery.

ASA Standard Monitors
There are 2 Basic Standards put out by the American Society of Anesthesiologists (ASA) that guide monitoring during any procedure or surgery require anesthesia. The first standard is “a qualified anesthesia personnel shall be present in the room throughout the conduct of all general anesthetics, regional anesthetics, and monitored anesthesia care”. The second standard is “during all anesthetics, the patient’s oxygenation, ventilation, circulation, and temperature shall be continually evaluated”. Continually is defined as “repeated regularly and frequent checks, no more than 5 minutes apart”. Let’s break down the 4 components further.

Neuraxial Anesthesia and Anticoagulants
This will be a review of when to hold and restart commonly seen anticoagulation in regards to epidural and spinal procedures, maintaining epidural catheters, and removing catheters.

The Brachial Plexus
This will provide an overview of the brachial plexus - it’s specific anatomy and how we can utilize various segments of the plexus to provide analgesia to specific areas in the upper extremity.

Multimodal Analgesia
This post discusses multiple options for analgesia that can be used to help reduce relying solely on one mechanism to control post-operative pain, such as with opiates.

Opiates
A review of terminology, types of opiates, routes of administration, and effects on organ systems and specific receptors

Local Anesthetics
This post covers the history of local anesthetics, their mechanism of action, and a review of their properties, additives, and toxicity.

Magnesium
This is a review of how magnesium is used in the obstetric population, typical dosing, contraindications, signs of overdose, and its antidote.

Preeclampsia
This is a review of types of hypertension during pregnancy, pathophysiology of preeclampsia, natural progression and complications, and treatment options.